 +91 96001 07057
+91 96001 07057 Sidharam Heart Clinic Adyar, Gandhi Nagar, Canal Bank Road, Opp.St.Louis School, Adyar, Chennai, Tamil Nadu 600020
Sidharam Heart Clinic Adyar, Gandhi Nagar, Canal Bank Road, Opp.St.Louis School, Adyar, Chennai, Tamil Nadu 600020 2 April, 2026
2 April, 2026
High-Risk Calcified RCA CTO PCI in a 76-Year-Old NSTEMI Patient With ADHF and Poor Surgical Targets
Treating severely calcified coronary artery disease in elderly, high-risk patients is rarely straightforward. These are the cases where success depends not just on one tool, but on careful step-by-step strategy, the ability to escalate appropriately, and the use of imaging-guided precision throughout the procedure.
We recently managed a 76-year-old multimorbid patient who presented with NSTEMI, acute decompensated heart failure, and reduced left ventricular systolic function with an LVEF of 37%. Coronary angiography showed diffuse, heavily calcified triple-vessel disease, with poor surgical targets, and the patient was considered a surgical turndown.
Among the most challenging lesions was a heavily calcified chronic total occlusion (CTO) of the right coronary artery (RCA). This case highlights the importance of persistence, lesion preparation, intravascular imaging, and procedural support in achieving a successful result in complex calcific PCI.



Post Rota with Calcium Fracture ☝️
A Patient Too High-Risk for Surgery, Yet Too Complex for Routine PCI
This was not a routine angioplasty case.
The patient had multiple layers of risk:
- advanced age
- multiple comorbidities
- NSTEMI presentation
- acute decompensated heart failure
- impaired LV function
- diffuse calcific triple-vessel disease
In such patients, every procedural choice matters. The goal is not just opening an artery, but doing so safely, effectively, and with enough plaque modification to allow durable stent expansion.
Because surgery was not a viable option, percutaneous revascularization became the only meaningful path forward.
Post Rota with Calcium Fracture ☝️
The Real Challenge Began After Wiring the CTO
The RCA lesion was a heavily calcified CTO, and as expected, the procedure demanded more than simple wire passage.
The lesion was first wired with a Fielder XTA, successfully negotiating the occlusion. However, in complex calcified CTO PCI, crossing the wire is often only the beginning. The next major problem was that the lesion remained extremely resistant to device passage.
A microcatheter could not cross.
An attempt was then made with a Nicnano 0.85 balloon, but even this could not cross the lesion. This immediately confirmed the severity of calcium burden and the rigid nature of the plaque architecture.
At that point, it became clear that this was not a lesion that would yield to conventional balloon-based escalation alone. The strategy had to shift toward plaque modification.
Post Stenting
Rotational Atherectomy as a Lesion-Modification Strategy
After exchanging to a dedicated rota wire, the next step was rotational atherectomy, performed in a segmental manner from the proximal RCA up to the crux.
This was the key turning point in the case.
In diffuse calcified disease, especially in CTO segments, adequate lesion preparation is what determines whether the rest of the PCI will be smooth or compromised. Without sufficient calcium modification, balloon expansion remains poor, device delivery is difficult, and final stent expansion may be suboptimal.
The aim of atherectomy here was not simply to “debulk,” but to create a more modifiable pathway through a long, resistant, heavily calcified vessel. In lesions like this, atherectomy plays a crucial role in transforming an undilatable artery into one that can be prepared properly for definitive PCI.
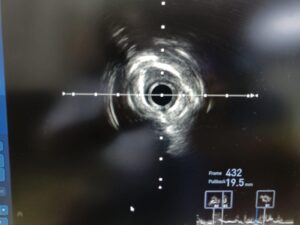
IVUS Revealed the True Calcium Burden
Following atherectomy, IVUS was performed, and this provided critical insight into the lesion morphology.
The imaging showed extensive severe calcium with mixed morphologies, confirming that the lesion was not only heavily calcified but also structurally complex. This is exactly why intracoronary imaging is so important in advanced calcium cases.
Angiography can suggest calcium. IVUS defines it.
It helps answer the questions that matter most:
- How deep and circumferential is the calcium?
- Has lesion modification been adequate?
- Is further preparation required before stenting?
- Will the vessel accept and expand a stent properly?
In this case, IVUS guided the next decision: further lesion optimization was still necessary.
Additional Plaque Preparation Before Stenting
After atherectomy, the vessel was further modified using an Apertha scoring balloon.
This was an important adjunctive step. In calcified coronary intervention, success often comes from combining techniques rather than relying on a single modality. Atherectomy helps create initial plaque modification, but scoring balloons can further improve lesion compliance, especially when calcium has mixed or irregular morphology.
This combined preparation allowed the lesion to become more receptive to stent delivery and expansion.
The procedure then progressed to long-segment stenting from proximal to distal RCA, with guide extension catheter support to facilitate equipment delivery across the treated vessel.
In long, calcified, complex RCA interventions, guide support often becomes a major determinant of success. Adequate support reduces friction, improves deliverability, and helps complete the procedure more efficiently in anatomy that would otherwise resist device passage.
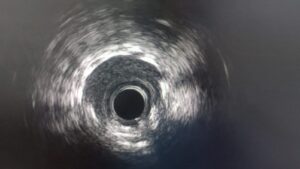
Final Result: Good Stent Expansion on IVUS
After stent implantation, post-PCI IVUS confirmed good stent expansion.
This is one of the most important takeaways from the case.
In severe calcific disease, the procedure should not be judged by angiographic appearance alone. The true procedural endpoint is not merely placing stents, but achieving:
- proper stent expansion
- good apposition
- full lesion coverage
- optimized vessel preparation before final deployment
That is why imaging remains central in modern complex PCI, particularly in calcified lesions and CTOs.
Good expansion in this setting reflects the value of the entire procedural sequence:
wire escalation, failed crossing attempts, atherectomy, imaging-guided assessment, additional scoring balloon modification, supported stent delivery, and final IVUS optimization.


Staged LM Bifurcation PCI
Hemodynamic Management in a Fragile Patient
Because of the patient’s reduced LV function, heart failure, and overall frailty, this was also a hemodynamically sensitive procedure.
During the intervention, the patient required transient pacing and minimal noradrenaline support. That underscores another major reality of high-risk PCI: technical success must always be matched by vigilant physiological support.
In complex coronary work, especially in elderly patients with low EF and diffuse disease, the procedure is not just about anatomy. It is equally about anticipating instability, managing it early, and safely carrying the patient through each stage of intervention.
Why This Case Matters
This case is a strong reminder that complex PCI in severely calcified coronary disease is often a procedural journey, not a single-step treatment.
The success came from:
- careful CTO wiring
- recognizing failure of standard device passage early
- timely escalation to plaque modification
- use of intravascular imaging
- adjunctive lesion preparation
- supported long-segment stenting
- continuous hemodynamic vigilance
In an elderly patient with NSTEMI, ADHF, impaired LV function, diffuse triple-vessel disease, and no good surgical option, achieving a good final result in a heavily calcified RCA CTO is deeply meaningful.
It reflects how contemporary interventional cardiology can offer a revascularization pathway even in patients once considered too complex or too high-risk.
About the Doctor
Dr. Dhamodaran K
Interventional Cardiologist
Dr. Dhamodaran K is a highly experienced Interventional Cardiologist known for his precision in diagnosis, evidence-based treatment approach, and patient-focused cardiac care. He specializes in the prevention, evaluation, and advanced interventional management of heart diseases, including coronary artery disease, angioplasty, stenting, heart failure management, and complex cardiac procedures.
With a strong commitment to early detection and preventive cardiology, Dr. Dhamodaran emphasizes comprehensive heart health evaluation, risk factor control, and personalized treatment planning. His clinical approach combines modern interventional techniques with compassionate patient care to ensure optimal outcomes.
Consultation Locations & Timings
Sidharam Multispeciality Clinic
Old #2, New #4, Canal Bank Road, Gandhi Nagar,
Adyar, Chennai, Tamil Nadu – 600020
Working Hours:
MON – THU : 06:00 PM – 09:00 PM
Apollo 247
Apollo Hospitals, Greams Road,
Chennai, Tamil Nadu
Working Hours:
MON – SAT : 10:00 AM – 04:00 PM