 +91 96001 07057
+91 96001 07057 Sidharam Heart Clinic Adyar, Gandhi Nagar, Canal Bank Road, Opp.St.Louis School, Adyar, Chennai, Tamil Nadu 600020
Sidharam Heart Clinic Adyar, Gandhi Nagar, Canal Bank Road, Opp.St.Louis School, Adyar, Chennai, Tamil Nadu 600020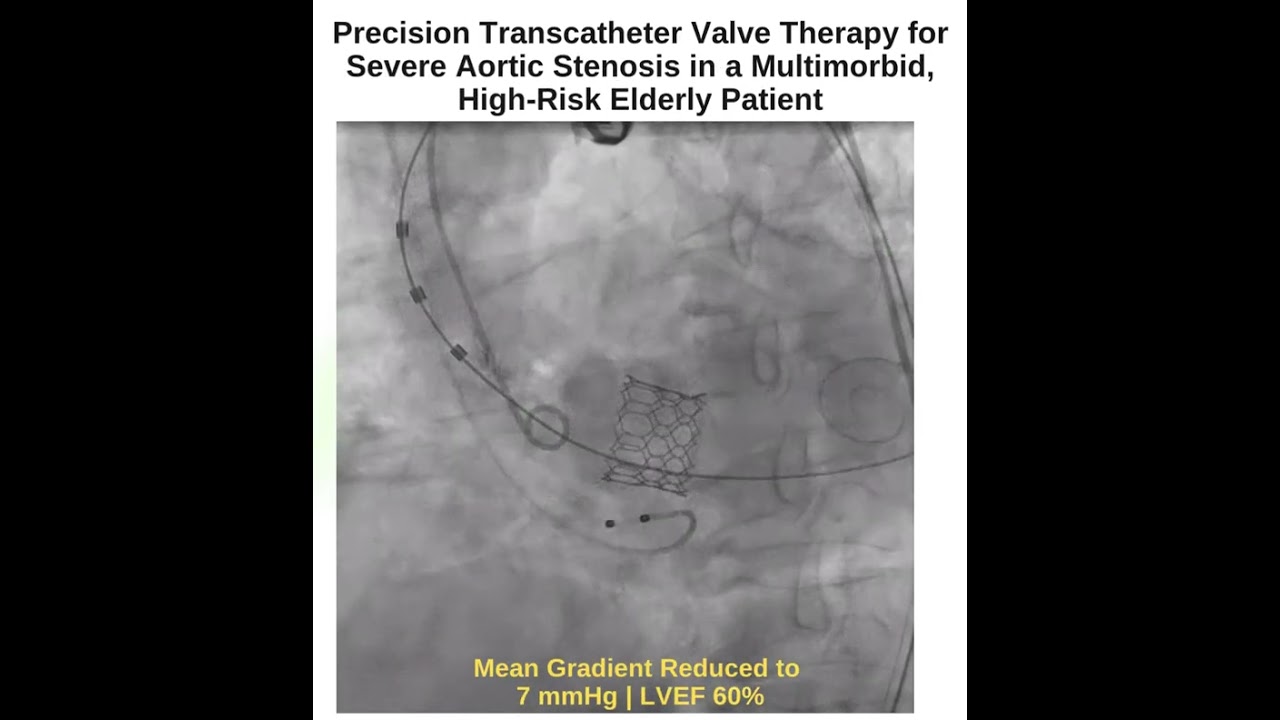 9 February, 2026
9 February, 2026
High-Risk TAVI in an Elderly Patient with Multiple Comorbidities: A Contemporary Approach to Complex Aortic Stenosis
Severe calcific aortic stenosis in elderly patients often presents one of the most complex decision-making challenges in modern cardiology. Advanced age, coupled with multiple systemic comorbidities, can make conventional surgical aortic valve replacement prohibitively risky. However, the evolution of transcatheter valve therapies has significantly changed outcomes for patients once considered untreatable.
This case involves an 87-year-old patient with symptomatic severe calcific aortic stenosis and a constellation of high-risk comorbidities, including advanced interstitial lung disease (UIP pattern) with severe pulmonary hypertension, biventricular dysfunction, and acute kidney injury following recent cardiogenic shock and intensive care admission. Despite these challenges, a carefully planned transfemoral transcatheter aortic valve implantation (TAVI) resulted in an excellent clinical and echocardiographic outcome.
This case highlights how contemporary TAVI, when guided by structured Heart Team decision-making, can provide meaningful benefit even in extremely high-risk elderly patients.
Understanding the Risk Profile in Advanced Aortic Stenosis
In elderly patients, severe aortic stenosis rarely exists in isolation. Degenerative valve disease often coexists with chronic pulmonary, renal, and ventricular dysfunction, all of which amplify procedural risk.
In this patient, several factors contributed to an exceptionally high surgical risk:
-
Advanced interstitial lung disease (UIP pattern) with severe pulmonary hypertension, significantly increasing peri-operative respiratory and right ventricular risk
-
Biventricular dysfunction, reducing physiological reserve
-
Recent cardiogenic shock and ICU stay, reflecting critical hemodynamic instability
-
Acute kidney injury, increasing vulnerability to contrast load and hypotension
Traditional open-heart surgery under cardiopulmonary bypass in such a setting would carry unacceptably high morbidity and mortality. This is precisely where transcatheter valve therapy has emerged as a life-saving alternative.
The Role of the Heart Team in High-Risk Decision-Making
High-risk TAVI is not simply a procedural choice—it is a multidisciplinary decision.
A detailed Heart Team evaluation is essential and typically includes interventional cardiologists, cardiac surgeons, cardiac anesthetists, imaging specialists, pulmonologists, and nephrologists. In this case, the Heart Team carefully weighed:
-
Expected survival and quality-of-life improvement
-
Reversibility of symptoms after relieving valvular obstruction
-
Procedural feasibility via transfemoral access
-
Risk of prolonged ventilation or renal deterioration
-
Patient and family goals of care
After thorough discussion, transfemoral TAVI was selected as the most appropriate and least invasive option offering potential clinical benefit.
Why Transfemoral TAVI Was the Preferred Strategy
Transfemoral TAVI has become the default access route whenever anatomically feasible, particularly in frail and elderly patients. Its advantages include:
-
Avoidance of sternotomy and cardiopulmonary bypass
-
Reduced procedural stress and inflammatory response
-
Lower risk of prolonged mechanical ventilation
-
Faster hemodynamic recovery
Given this patient’s severe lung disease and recent critical illness, minimizing procedural invasiveness was a key priority.
Step-by-Step Approach to the High-Risk TAVI Procedure
1. Pre-Procedural Planning and Imaging
Comprehensive CT angiography was performed to assess aortic annular dimensions, valve calcification pattern, coronary heights, and vascular access suitability. Careful sizing was essential to minimize the risk of paravalvular leak or annular injury.
2. Valve Selection
A 21.5 mm Myval transcatheter heart valve was selected based on annular measurements and anatomical considerations. The Myval platform offers precise sizing options, which is particularly valuable in complex anatomies.
3. Anesthesia Strategy
Given the pulmonary risk, anesthesia planning focused on minimizing respiratory compromise. Hemodynamic monitoring was meticulous, with careful fluid and vasopressor management to protect both ventricular and renal function.
4. Transfemoral Access and Valve Deployment
The procedure was performed via transfemoral access under controlled conditions. The valve was accurately positioned and deployed across the native calcified aortic valve, achieving immediate hemodynamic improvement.
5. Post-Deployment Assessment
Immediate post-implant echocardiography confirmed excellent valve expansion and function, with no significant paravalvular regurgitation.
Post-Procedure Results and Clinical Outcome
Post-procedure transthoracic echocardiography demonstrated:
-
Excellent valve performance
-
Mean transvalvular gradient of 7 mmHg
-
Preserved left ventricular systolic function (LVEF 60%)
Clinically, the patient showed hemodynamic stabilization and symptomatic improvement, validating the Heart Team’s decision despite the extremely high-risk profile.
Why This Case Matters in Modern Cardiology
This case reflects a broader shift in the management of structural heart disease. Advanced age and multiple comorbidities are no longer absolute barriers to intervention. Instead, success depends on:
-
Individualized patient selection
-
Detailed anatomical and physiological assessment
-
Multidisciplinary collaboration
-
Careful procedural planning
High-risk TAVI is not about pushing boundaries indiscriminately—it is about offering thoughtful, evidence-based care tailored to each patient’s unique risk profile.
Conclusion
In extremely high-risk elderly patients with severe aortic stenosis, contemporary transcatheter valve therapy offers a viable and often transformative treatment option. This case demonstrates that even in the presence of advanced lung disease, pulmonary hypertension, ventricular dysfunction, and recent critical illness, carefully planned transfemoral TAVI can achieve excellent outcomes.
With the right expertise, technology, and multidisciplinary approach, meaningful clinical benefit is possible where traditional surgery is no longer an option.
Treating Specialist
Dr. Dhamodaran K
Senior Interventional Cardiologist
Expert in complex coronary and structural heart interventions, including high-risk TAVI procedures.
Consultation Locations
Sidharam Multispeciality Clinic
Old #2, New #4, Canal Bank Road,
Gandhi Nagar, Adyar,
Chennai, Tamil Nadu 600020
Working Hours
MON – THU: 06:00 PM – 09:00 PM
Apollo 247
Apollo Hospitals, Greams Road,
Chennai
Working Hours
MON – SAT: 10:00 AM – 04:00 PM