 +91 96001 07057
+91 96001 07057 Sidharam Heart Clinic Adyar, Gandhi Nagar, Canal Bank Road, Opp.St.Louis School, Adyar, Chennai, Tamil Nadu 600020
Sidharam Heart Clinic Adyar, Gandhi Nagar, Canal Bank Road, Opp.St.Louis School, Adyar, Chennai, Tamil Nadu 600020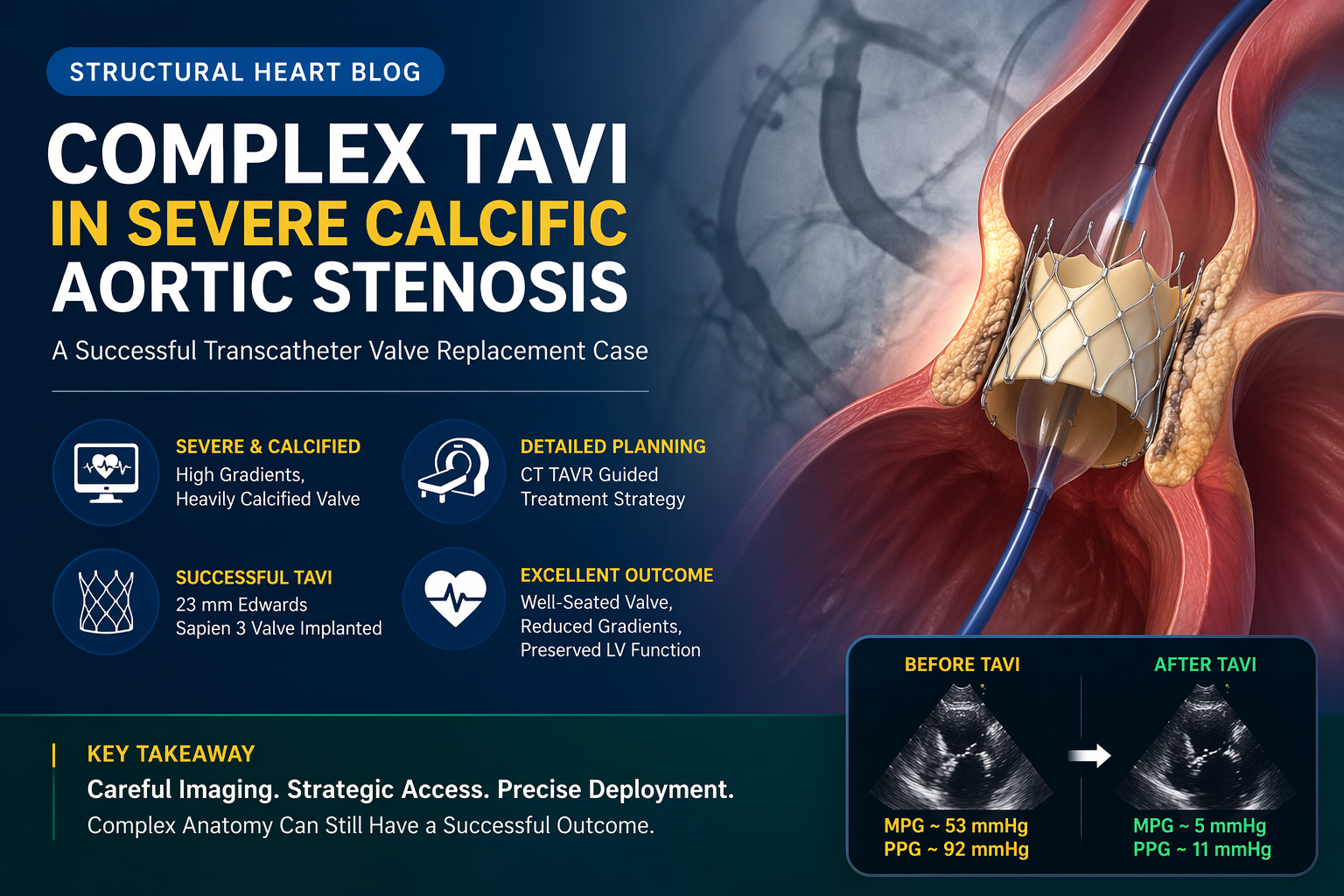 17 April, 2026
17 April, 2026
Complex TAVI in Severe Calcific Aortic Stenosis: A Successful Structural Heart Intervention
Severe aortic stenosis is a serious heart valve condition in which the aortic valve becomes narrowed, stiff, and unable to open properly. The aortic valve plays a vital role in allowing blood to flow from the heart’s main pumping chamber, the left ventricle, into the aorta and then to the rest of the body. When this valve becomes severely narrowed, the heart has to work much harder to pump blood forward.
Over time, this increased pressure load can lead to symptoms such as breathlessness, chest pain, fatigue, dizziness, fainting episodes, and heart failure. In elderly patients, severe aortic stenosis is often caused by progressive calcium buildup on the valve leaflets. This makes the valve thick, rigid, and restricted.
Traditionally, severe aortic stenosis was treated with open-heart surgical valve replacement. However, many patients, especially elderly individuals or those with multiple medical conditions, may not be ideal candidates for conventional surgery. Transcatheter Aortic Valve Implantation, commonly known as TAVI, has emerged as a major advancement in the treatment of severe aortic stenosis. It allows valve replacement through a catheter-based approach, most commonly through the femoral artery in the leg, without the need for open-heart surgery.
This case highlights a complex TAVI procedure performed in a 70-year-old gentleman with severe calcific aortic stenosis, dense bulky valve calcification, high valve gradients, and coexisting peripheral arterial disease. Despite the technical challenges, careful assessment, strategic access planning, and precise valve deployment resulted in a successful outcome.
Understanding Severe Calcific Aortic Stenosis
The aortic valve normally opens and closes with every heartbeat. When the heart contracts, the valve opens to allow blood to leave the heart. When the heart relaxes, the valve closes to prevent blood from leaking backward.
In aortic stenosis, the valve does not open fully. This restricts blood flow and creates pressure buildup inside the heart. When the stenosis becomes severe, the left ventricle must generate much higher pressure to push blood through the narrowed valve. Over time, this can cause thickening of the heart muscle, known as left ventricular hypertrophy.
Calcific aortic stenosis usually develops gradually over many years. Calcium deposits accumulate on the valve leaflets, making them stiff and less mobile. As the valve opening becomes smaller, patients may begin to experience symptoms during physical activity. These symptoms may include shortness of breath, chest discomfort, reduced exercise tolerance, dizziness, or swelling due to heart failure.
Once symptoms appear in severe aortic stenosis, timely treatment becomes very important. Medication may help manage symptoms temporarily, but it cannot open the narrowed valve. Valve replacement remains the definitive treatment.
Case Overview
A 70-year-old gentleman presented with progressive exertional dyspnea and angina. Exertional dyspnea means breathlessness during activity, while angina refers to chest pain or discomfort caused by reduced blood flow or increased strain on the heart. These symptoms suggested that the aortic valve narrowing was significantly affecting the patient’s heart function and daily life.
Echocardiography revealed severe aortic stenosis. The aortic valve was heavily calcified and restricted, meaning the valve leaflets were thickened, stiff, and unable to open properly. The valve gradients were significantly elevated, with a mean pressure gradient of approximately 53 mmHg and a peak pressure gradient of approximately 92 mmHg. These high gradients confirmed the severity of obstruction across the valve.
The patient also had concentric left ventricular hypertrophy, which occurs when the heart muscle thickens in response to chronic pressure overload. Fortunately, the left ventricular systolic function was preserved, meaning the heart’s pumping ability remained intact.
Further evaluation with CT TAVR protocol showed a tricuspid aortic valve with dense, bulky calcification. The calcium score was approximately 2494, indicating a high calcium burden and a high-risk anatomical subset for intervention. The patient also had coexisting peripheral arterial disease, which made vascular access planning more challenging.
Why This TAVI Procedure Was Complex
Although TAVI is a minimally invasive procedure, not every case is simple. The success of the procedure depends heavily on the patient’s anatomy, the condition of the valve, calcium distribution, vascular access, and overall clinical risk.
In this case, the aortic valve had dense and bulky calcification. Heavy calcification can create multiple challenges during TAVI. It can make it difficult to cross the valve, affect the expansion of the new valve, increase the risk of incomplete sealing, and lead to paravalvular leak. If calcium is unevenly distributed, it may also affect the stability and positioning of the implanted valve.
Another important complexity was peripheral arterial disease. Since transfemoral TAVI is usually performed through the femoral artery, the condition of the leg arteries is extremely important. Narrowed, calcified, or diseased blood vessels can make it difficult to safely advance the catheter and valve delivery system to the heart.
Because of these challenges, careful planning was essential. The heart team needed to assess not only the valve but also the access route, device size, calcification pattern, and deployment strategy. In this case, right femoral artery access with surgical cutdown was chosen to support a controlled and safe procedure.
Role of Echocardiography in Diagnosis
Echocardiography is one of the most important tests for diagnosing aortic stenosis. It provides detailed information about valve structure, valve movement, blood flow velocity, pressure gradients, heart chamber size, wall thickness, and pumping function.
In this patient, echocardiography confirmed severe aortic stenosis. The valve was heavily calcified and restricted. The high mean and peak pressure gradients showed that blood flow across the valve was severely obstructed. Echocardiography also showed concentric left ventricular hypertrophy, which reflected the long-standing pressure overload on the heart.
Preserved left ventricular systolic function was an encouraging finding. It indicated that although the heart was under significant pressure stress, its pumping ability was still maintained. This made timely intervention even more important to prevent further deterioration.
Importance of CT TAVR Protocol
CT TAVR protocol plays a critical role in planning a successful TAVI procedure. It helps the team evaluate the valve anatomy, annulus size, aortic root, coronary artery height, calcium distribution, and vascular access route.
In this case, CT imaging demonstrated a tricuspid aortic valve with dense, bulky calcification and a calcium score of approximately 2494. This finding was important because high calcium burden can increase procedural complexity. It can influence valve sizing, valve expansion, risk of paravalvular leak, and overall procedural strategy.
CT imaging also helped assess the peripheral arteries. Since the patient had peripheral arterial disease, the team needed to carefully evaluate whether transfemoral access was feasible and safe. This step was crucial in planning the right access approach and minimizing vascular complications.
The TAVI Procedure
The patient underwent successful transfemoral TAVI using right femoral artery access with surgical cutdown. A 23 mm Edwards Sapien 3 valve was implanted.
During TAVI, a replacement valve is mounted on a catheter and advanced through the blood vessels to the heart. Once the valve reaches the diseased aortic valve, it is positioned carefully and deployed. The new valve pushes the diseased native valve leaflets aside and begins functioning immediately.
In heavily calcified valves, positioning and deployment require exceptional precision. The valve must be placed accurately to ensure proper sealing, stable anchoring, and effective blood flow. In this case, despite the challenging anatomy and access considerations, the procedure was executed successfully with optimal device positioning and deployment.
Post-Procedure Result
Post-procedure echocardiography showed a well-seated bioprosthetic valve. This means the implanted valve was positioned correctly and functioning well.
There was a significant reduction in transvalvular gradients. The mean pressure gradient reduced from approximately 53 mmHg before the procedure to approximately 5 mmHg after the procedure. The peak pressure gradient reduced from approximately 92 mmHg to approximately 11 mmHg. This dramatic reduction showed that the obstruction across the aortic valve had been successfully relieved.
The patient had mild paravalvular leak, which can occur after TAVI, especially in heavily calcified valves. Importantly, the left ventricular function remained preserved.
Overall, the outcome was highly satisfactory, especially considering the technical difficulty of the case.
Why TAVI Is Important in Modern Cardiac Care
TAVI has transformed the treatment of severe aortic stenosis. It offers a less invasive alternative to open-heart surgery for selected patients. This is particularly important for elderly patients, patients with high surgical risk, and those with complex medical conditions.
The benefits of TAVI may include smaller access wounds, reduced need for open surgery, shorter recovery time, and faster return to normal activities. However, patient selection remains extremely important. Not every patient with severe aortic stenosis is automatically suitable for TAVI.
The decision must be based on a complete assessment of the patient’s symptoms, valve anatomy, age, surgical risk, vascular access, other medical conditions, and long-term treatment goals. A multidisciplinary heart team approach is essential to choose the safest and most effective treatment strategy.
Key Lessons From This Case
This case highlights the importance of detailed pre-procedure planning in complex structural heart interventions. Severe calcification, high gradients, and peripheral arterial disease can make TAVI technically demanding. However, with careful imaging and a well-planned strategy, successful outcomes are possible.
The case also demonstrates the value of multimodality imaging. Echocardiography helped confirm the severity of aortic stenosis, while CT TAVR protocol provided essential anatomical information for valve sizing, calcium assessment, and access planning.
Another important lesson is the role of precise device selection and deployment. In heavily calcified valves, choosing the right valve size and deploying it accurately are critical to achieving good results and minimizing complications.
Conclusion
This complex TAVI case in severe calcific aortic stenosis demonstrates the power of advanced structural heart intervention. A 70-year-old gentleman with progressive breathlessness and angina was diagnosed with severe aortic stenosis, high valve gradients, dense bulky calcification, and peripheral arterial disease.
The case required detailed echocardiographic and CT-based evaluation, careful access planning, and precise device deployment. The patient successfully underwent transfemoral TAVI using a 23 mm Edwards Sapien 3 valve through right femoral artery access with surgical cutdown.
Post-procedure echocardiography confirmed a well-seated valve, significant reduction in gradients, mild paravalvular leak, and preserved left ventricular function. This outcome reflects the importance of expertise, planning, and precision in managing complex valve disease.
For patients with severe aortic stenosis, especially those with challenging anatomy or higher surgical risk, TAVI can offer an effective and minimally invasive treatment option when performed by an experienced heart team.
FAQs
1. What is TAVI?
TAVI stands for Transcatheter Aortic Valve Implantation. It is a minimally invasive procedure used to replace a narrowed aortic valve without traditional open-heart surgery.
2. What is severe aortic stenosis?
Severe aortic stenosis is a condition where the aortic valve becomes very narrow and restricts blood flow from the heart to the rest of the body.
3. What causes calcific aortic stenosis?
Calcific aortic stenosis is usually caused by calcium buildup on the valve leaflets over time. This makes the valve stiff, thick, and unable to open properly.
4. What are the symptoms of severe aortic stenosis?
Common symptoms include breathlessness, chest pain, fatigue, dizziness, fainting, reduced exercise tolerance, and signs of heart failure.
5. Why was this case considered complex?
This case was complex because the patient had dense bulky valve calcification, very high valve gradients, and peripheral arterial disease, all of which made the procedure more technically challenging.
6. What is the role of CT before TAVI?
CT helps evaluate the valve anatomy, calcium burden, annulus size, aortic root, coronary height, and blood vessel access route. It is essential for planning the procedure safely.
7. What is a valve gradient?
A valve gradient is the pressure difference across the valve. A high gradient means the heart has to work harder to push blood through the narrowed valve.
8. What valve was used in this case?
A 23 mm Edwards Sapien 3 valve was used for the TAVI procedure.
9. What does mild paravalvular leak mean?
Mild paravalvular leak means a small amount of blood is passing around the new valve rather than through it. It can occur after TAVI, especially in heavily calcified valves.
10. What was the outcome of this case?
The outcome was successful. The new valve was well seated, the gradients reduced significantly, left ventricular function remained preserved, and only mild paravalvular leak was noted.
11. Is TAVI suitable for every patient?
No. TAVI suitability depends on the patient’s age, symptoms, valve anatomy, surgical risk, vascular access, and overall health condition.
12. Why is heart team evaluation important?
A heart team evaluates all aspects of the patient’s condition and decides whether TAVI or surgery is the best treatment option. This approach helps improve safety and outcomes.