 +91 96001 07057
+91 96001 07057 Sidharam Heart Clinic Adyar, Gandhi Nagar, Canal Bank Road, Opp.St.Louis School, Adyar, Chennai, Tamil Nadu 600020
Sidharam Heart Clinic Adyar, Gandhi Nagar, Canal Bank Road, Opp.St.Louis School, Adyar, Chennai, Tamil Nadu 600020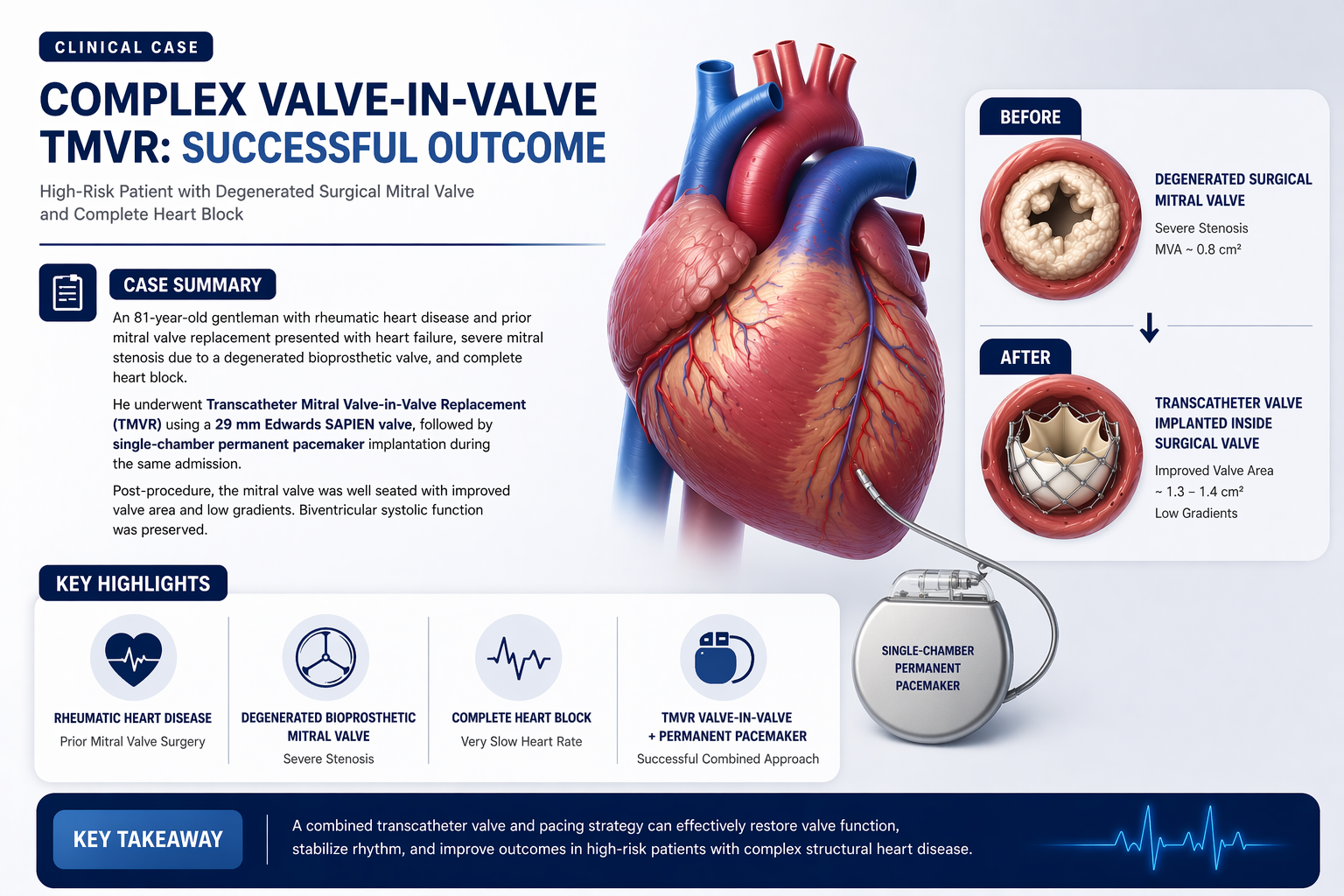 9 April, 2026
9 April, 2026
Complex Valve-in-Valve TMVR in a Post-Surgical Rheumatic Heart Disease Patient
Heart valve disease continues to pose a major long-term challenge in patients with rheumatic heart disease, especially in those who have already undergone previous valve surgery. Although surgically implanted bioprosthetic valves can provide many years of clinical benefit, structural valve degeneration may eventually lead to recurrent obstruction or regurgitation, progressive heart failure, pulmonary hypertension, arrhythmias, and substantial functional decline.
In elderly patients with prior sternotomy, repeat open-heart surgery is often associated with significant risk. That is where contemporary structural heart interventions offer an important alternative. Transcatheter Mitral Valve-in-Valve Replacement, commonly referred to as TMVR, allows a new transcatheter valve to be implanted inside a failing surgical bioprosthesis without the trauma of redo valve surgery.
The case discussed here illustrates how a carefully planned, imaging-guided, technology-driven approach can be lifesaving in a high-risk elderly patient with multiple simultaneous cardiac challenges. It also demonstrates how structural intervention and rhythm management can be successfully combined in the same admission when the clinical situation demands it.
Patient Background and Clinical Presentation
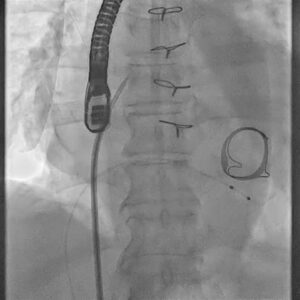
Figure 1. Baseline fluoroscopic procedural still showing prior surgical mitral prosthesis region and catheter setup.
This case involved an 81-year-old gentleman with a history of rheumatic heart disease who had previously undergone surgical mitral valve replacement and tricuspid valve repair on 23 July 2014. During that earlier operation, he received a 29 mm Perimount Edwards Lifesciences bioprosthetic mitral valve along with a TARP 29 St. Jude Medical annuloplasty ring.
He presented with symptomatic bradycardia and decompensated heart failure. Evaluation revealed degeneration of the mitral bioprosthesis with severe prosthetic stenosis and a mitral valve area of approximately 0.8 cm². Additional findings included marked biatrial enlargement, moderate tricuspid regurgitation, and pulmonary hypertension. During admission, he developed complete heart block with a ventricular rate of around 25 beats per minute, requiring urgent temporary pacing and intensive haemodynamic stabilisation.
This combination of a failing prosthetic mitral valve, worsening heart failure, pulmonary vascular burden, and life-threatening conduction disturbance made the clinical scenario exceptionally complex.
Why Redo Surgery Was Not the Best Option
Redo cardiac surgery in elderly patients is technically demanding and can carry markedly higher perioperative risk than a first operation. Scar tissue from prior surgery, frailty, pulmonary hypertension, decompensated haemodynamics, and associated conduction abnormalities all contribute to procedural complexity.
In this patient, repeat open-heart surgery would likely have involved a difficult re-entry, a prolonged procedure, and a higher chance of postoperative complications. Given his age, prior mitral valve surgery, current decompensated status, and complete heart block, a minimally invasive transcatheter approach offered a more pragmatic and safer strategy.
The decision to proceed with TMVR was therefore based on anatomy, previous surgical history, overall operative risk, and the need for timely intervention.
What Valve-in-Valve TMVR Means
Valve-in-valve TMVR involves delivering a new transcatheter heart valve into a previously implanted but now degenerated surgical bioprosthetic mitral valve. Instead of removing the old valve, the new prosthesis is carefully positioned within it to restore functional opening and improve haemodynamics.
In this case, the treating team used a 29 mm Edwards SAPIEN valve. Successful use of this platform in the mitral position requires precise sizing, careful imaging interpretation, controlled deployment, and close assessment of post-implant gradients and valve position.
For appropriately selected patients, this method can provide relief from severe prosthetic mitral stenosis while avoiding the burden of another open surgical procedure.
Why This Case Was Especially Challenging
Several features contributed to the complexity of this intervention. First, the patient had rheumatic heart disease and prior valve surgery, which often create anatomically and haemodynamically difficult scenarios. Second, the existing mitral bioprosthesis had severely degenerated, resulting in critical obstruction of blood flow. Third, pulmonary hypertension and moderate tricuspid regurgitation indicated that the consequences of the failing valve were already affecting the right side of the heart.
Perhaps most importantly, the patient developed complete heart block with profound bradycardia. That meant the team had to address not only the structural valve problem but also a major electrical conduction disturbance. In practical terms, both haemodynamic restoration and dependable rhythm support were necessary to achieve a stable clinical recovery.
Cases like this highlight the value of an integrated heart-team approach, where interventional cardiology, imaging, pacing expertise, and critical care management work together in real time.
Procedural Planning and Imaging Guidance
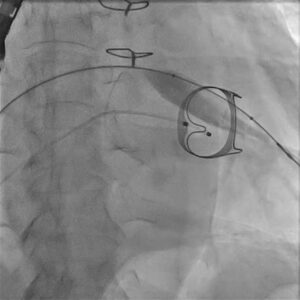
Figure 2. Fluoroscopic still during transcatheter valve positioning across the degenerated surgical mitral bioprosthesis.
A successful TMVR procedure begins well before the catheter enters the body. Careful case planning is essential to understand the dimensions of the prior surgical valve, the feasibility of transcatheter placement, access route considerations, and the risk of procedural complications. In complex valve-in-valve procedures, fluoroscopy and echocardiographic guidance are central to accurate positioning and deployment.
In this patient, the old surgical prosthesis had to be crossed and assessed with precision. The transcatheter valve system was then advanced and aligned within the failed bioprosthetic mitral valve. Exact orientation and deployment depth are crucial, because even a small positional error can affect prosthesis seating, gradients, and overall function.
The procedural stills from the uploaded case video help visualise this journey from catheter setup to valve positioning, expansion, and final stabilisation.
The Valve-in-Valve TMVR Procedure
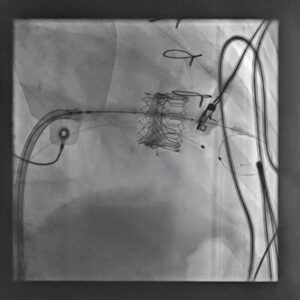
Figure 3. Expanded valve-in-valve prosthesis after deployment within the prior surgical mitral valve.
The patient underwent Transcatheter Mitral Valve-in-Valve Replacement using a 29 mm Edwards SAPIEN valve. Under advanced fluoroscopic and imaging guidance, the new valve was carefully positioned within the failing surgical mitral bioprosthesis and deployed in a controlled manner.
The objective was to create a well-seated valve-in-valve construct that would relieve the severe mitral obstruction, improve forward flow, and reduce transvalvular gradients. Controlled deployment is especially important in the mitral position, where anatomy, angle, and prior prosthetic material can influence the final result.
Following successful valve implantation, attention then shifted to the rhythm issue. During the same hospital admission, the patient underwent single-chamber permanent pacemaker implantation using a Medtronic–Vitatron system, thereby addressing the complete heart block and providing reliable ventricular pacing support.
Post-Procedural Outcome
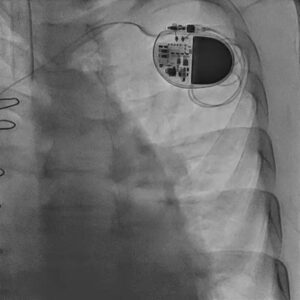
Figure 4. Post-procedural chest fluoroscopic image showing the implanted permanent pacemaker system.
Post-procedural echocardiography confirmed a well-seated mitral valve-in-valve prosthesis with clear haemodynamic improvement. The mitral valve area increased to approximately 1.3 to 1.4 cm², and residual transvalvular gradients were low. Biventricular systolic function remained preserved.
From a clinical standpoint, this represented successful restoration of mitral valve performance in a patient who had presented in heart failure with a critically stenosed prosthesis. The permanent pacemaker also ensured electrical stability after complete heart block, completing the second major component of his treatment.
Together, these outcomes underscore how coordinated transcatheter therapy and pacing intervention can change the trajectory of care in elderly high-risk patients.
Why This Case Matters
This case is important because it reflects a real-world structural heart challenge that would once have carried very limited options. Many elderly patients with prior valve surgery are not ideal candidates for repeat sternotomy, yet their symptoms and haemodynamics may deteriorate rapidly once a bioprosthetic valve fails.
Valve-in-valve TMVR provides a minimally invasive option that can offer meaningful haemodynamic recovery, symptom improvement, and avoidance of redo open surgery. When performed with careful planning and appropriate technology, it can be both safe and highly effective.
This case also demonstrates that advanced structural interventions are not isolated procedures. They often need to be integrated with rhythm management, temporary support strategies, imaging expertise, and critical inpatient care. That broader systems-based approach is one of the hallmarks of modern high-end cardiovascular treatment.
Conclusion
The successful management of this 81-year-old post-surgical rheumatic heart disease patient highlights the power of modern transcatheter therapy in high-risk structural heart disease. Faced with severe degeneration of a surgical mitral bioprosthesis, decompensated heart failure, pulmonary hypertension, and complete heart block, the treating team adopted a combined minimally invasive strategy that addressed both the valve lesion and the conduction problem.
Transcatheter Mitral Valve-in-Valve Replacement using a 29 mm Edwards SAPIEN valve, followed by single-chamber permanent pacemaker implantation using a Medtronic–Vitatron system, resulted in excellent procedural and echocardiographic outcomes. The valve was well seated, haemodynamics improved, gradients remained low, and ventricular function was preserved.
For patients considered too high risk for redo surgery, this case stands as a strong example of how precision-guided structural intervention can deliver durable clinical benefit and restore stability when conventional options are less suitable.
Frequently Asked Questions
- What is TMVR? TMVR stands for Transcatheter Mitral Valve Replacement. It is a minimally invasive method of treating mitral valve disease in selected patients without performing conventional open-heart surgery.
- What does valve-in-valve TMVR mean? It means placing a new transcatheter valve inside a previously implanted surgical bioprosthetic valve that has degenerated over time.
- Why do surgical tissue valves fail? Bioprosthetic valves can gradually degenerate, calcify, narrow, or leak over time. This process is called structural valve degeneration.
- Why was open surgery avoided in this case? Because the patient was elderly, had prior cardiac surgery, decompensated heart failure, pulmonary hypertension, and complete heart block, redo surgery carried substantially higher risk.
- Which transcatheter valve was used? A 29 mm Edwards SAPIEN valve was used for the mitral valve-in-valve procedure.
- Why was a pacemaker required? The patient developed complete heart block with a very slow ventricular rate, so permanent pacing was required to maintain a stable heart rhythm.
- What was the result after TMVR? Post-procedural echocardiography showed a well-seated valve-in-valve prosthesis, improved mitral valve area, low gradients, and preserved biventricular systolic function.
- Who may benefit from valve-in-valve TMVR? Patients with a failing surgical bioprosthetic mitral valve who are considered high risk for repeat open-heart surgery may benefit after detailed structural heart evaluation.
Doctor Details
Dr. Dhamodaran K
Interventional Cardiologist
Dr. Dhamodaran K is a highly experienced Interventional Cardiologist known for his precision in diagnosis, evidence-based treatment approach, and patient-focused cardiac care. He specializes in the prevention, evaluation, and advanced interventional management of heart diseases, including coronary artery disease, angioplasty, stenting, heart failure management, and complex cardiac procedures.
With a strong commitment to early detection and preventive cardiology, Dr. Dhamodaran emphasizes comprehensive heart health evaluation, risk factor control, and personalized treatment planning. His clinical approach combines modern interventional techniques with compassionate patient care to ensure optimal outcomes.
Consultation Locations & Timings
Sidharam Multispeciality Clinic
Old #2, New #4, Canal Bank Road, Gandhi Nagar,
Adyar, Chennai, Tamil Nadu – 600020
Working Hours:
MON – THU: 06:00 PM – 09:00 PM
Apollo 247
Apollo Hospitals, Greams Road,
Chennai, Tamil Nadu
Working Hours:
MON – SAT: 10:00 AM – 04:00 PM
Disclaimer: This blog is for educational and awareness purposes only. Treatment decisions should always be made after consultation with a qualified cardiologist based on individual clinical evaluation.